Dieser Beitrag ist auch verfügbar auf:
![]() Deutsch
Deutsch
Electrode placement is not a one-size-fits-all solution: Why individual adaptation is key to the success of treatmentT
In microcurrent therapy, we repeatedly encounter the same pattern: an electrode configuration is demonstrated in a seminar, documented in a photograph – and then applied unchanged to every patient with similar symptoms. This approach is understandable, as it saves time and initially seems practical. In practice, however, it often leads to a problem for which a pithy term has become established in our seminars: ‘Copy and paste quickly becomes copy and waste.’
Why a standard electrode configuration does not always work
Let’s take a classic example: chronic knee pain. The obvious reaction is to place electrodes directly on the knee – locally, in a focused manner, exactly where the pain is felt. This strategy can work extremely well, for instance post-operatively or following a clearly definable injury where the cause lies unequivocally within the treated tissue.
It becomes more difficult when the knee pain actually originates from a biomechanical chain – for example, from the hip, the ankle or the foot. In this case, the symptom manifests in the knee without the cause being there. A purely local treatment may then fail to achieve a lasting effect even over many sessions, regardless of how correctly the electrodes themselves were positioned.
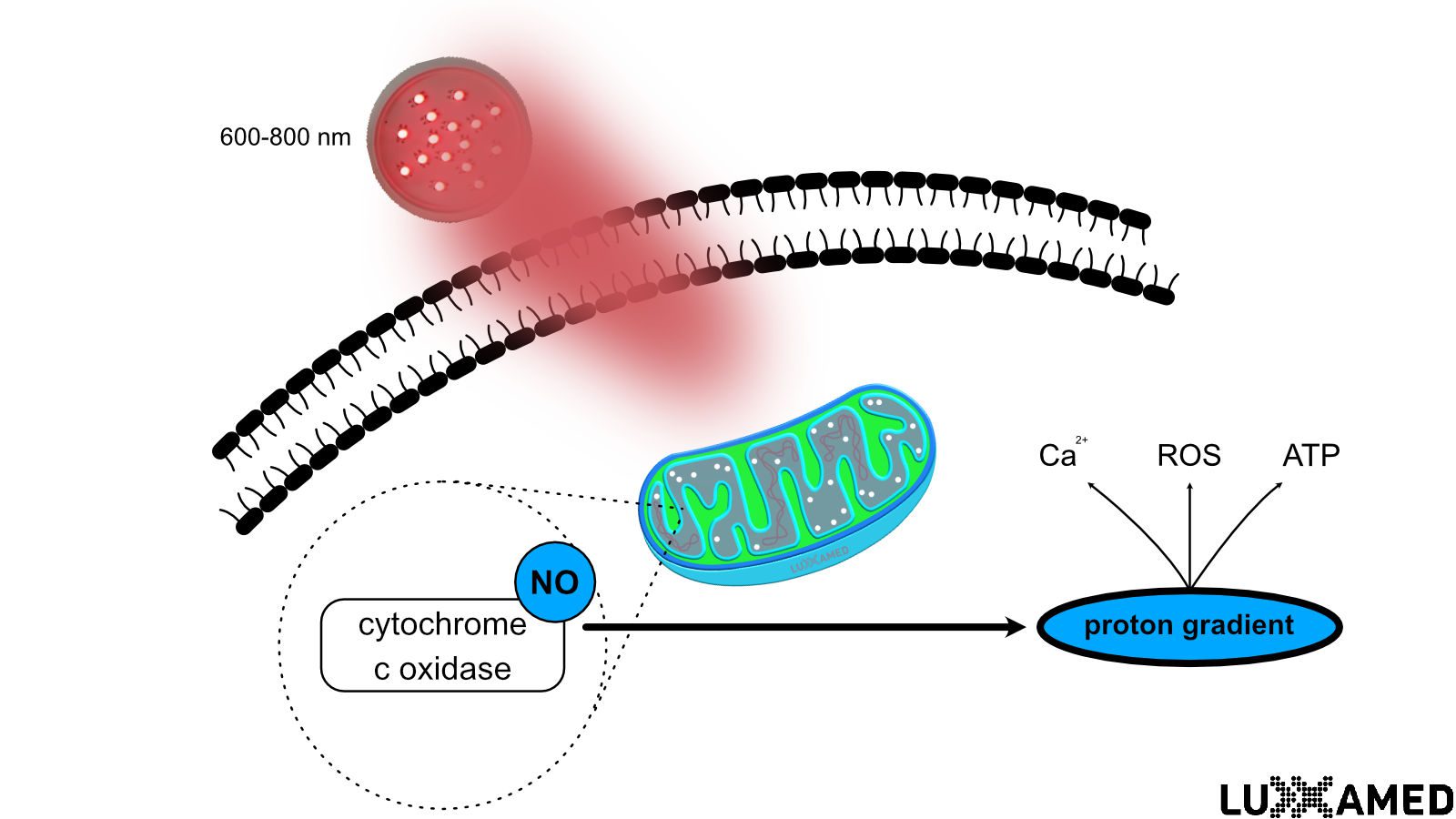
The reason for this lies in the physiological mechanism of action of microcurrent. Unlike conduction anaesthesia, which interrupts the transmission of stimuli within a nerve regardless of the site of origin, microcurrent locally influences the metabolic processes within the treated tissue itself – such as ATP production, membrane transport and cell communication. If the cause lies outside the treated area, the desired effect will not be achieved.
The fact that pain can be perceived in a different location to where it originates is also well documented in pain research. Mense (2008) describes how sustained stimulation of pain receptors in a muscle can lead to central sensitisation in the spinal cord, causing pain to be projected to a different region of the body from that in which the actual source of the stimulus lies. Fascia research also provides an anatomical explanation: Myers (2004), with his concept of ‘Anatomy Trains’, describes continuous myofascial chains extending across several joints, and recent biomechanical studies show that movements in the ankle joint propagate measurably as far as the thigh muscles.
Three conceptual models, one tool
Over the years, various strategies have become established in clinical practice; all utilise the same device but are based on different underlying assumptions:
The local, symptom-oriented approach (historically referred to as the ‘DaWoS method’ – ‘where it hurts’) is particularly suitable for clearly definable causes, such as in the post-operative period. A cellular mechanism of action for this has now been well described: Lee et al. (2024) were able to show that microcurrent stimulation of chondrocytes inhibits the pro-inflammatory NF-κB signalling cascade and, in an animal model, reduces the degradation of the subchondral bone structure in osteoarthritis.
The systemic approach takes a causal approach, treating not the site of the symptom but the underlying chain of events – often in combination with manual therapy or osteopathic techniques. McMakin (2004) documented a significant and sustained reduction in pain in treatment-resistant patients with chronic myofascial back pain following a correspondingly broader application of microcurrent therapy. A controlled study on myofascial pain syndrome of the cervical spine also showed a reduction in pain scores from 7 to 3.8 points on the visual analogue scale within two weeks (Iodice et al., 2016).
The regulatory concept goes one step further and considers three fundamental conditions for healthy cellular regulation: the supply and removal of nutrients and waste products via the semi-permeable cell membrane, the provision of sufficient energy, and the coordination of cellular processes. According to this model, if these conditions are met, the basis for a pathological tissue condition is eliminated.
The Tensegrity Model as an Explanatory Framework
Why does a systemic, aetiological approach work at all? One answer is provided by the Tensegrity model, a concept drawn from architecture and biomechanics that describes structures whose stability is based not on rigid connections but on a balanced interplay of tensile and compressive forces. Applied to the human body, this means that the membrane matrix, cytoskeleton and extracellular matrix form a continuously interconnected system in which a mechanical change at one point – such as an old injury to the ankle – can manifest as a symptom at a completely different point, such as the knee. This concept is also well established in the current specialist literature on fascia research, which describes the fascial system as a three-dimensional continuum through which mechanical tension is distributed throughout the body.
What this means in practice
The implication for clinical practice is not to regard any one of the three schools of thought as the sole correct approach, but rather to make a conscious decision in each case: can the cause be localised, or does the symptom form part of a chain that originates elsewhere? A thorough medical history – including any factors that may have been overlooked, such as old scars or previous trauma – and a willingness to change strategy if the initial approach proves ineffective are more important than the exact replication of a template. The four galvanically isolated channels of the Luxxamed devices also allow local and systemic strategies to be combined simultaneously where necessary.
Sources
Iodice, P., Lessiani, G., Franzone, G., & Pezzulo, G. (2016). Efficacy of pulsed low-intensity electric neuromuscular stimulation in reducing pain and disability in patients with myofascial syndrome. Journal of Biological Regulators and Homeostatic Agents, 30(2), 615–620.
Lee, M., Lee, H., Chung, H., Lee, J.-H., Kim, D., Cho, S., Kim, T.-J., & Kim, H. S. (2024). Micro-current stimulation could inhibit IL-1β-induced inflammatory responses in chondrocytes and protect knee bone cartilage from osteoarthritis. Biomedical Engineering Letters, 14(4), 801–812.
McMakin, C. R. (2004). Microcurrent therapy: a novel treatment method for chronic low back myofascial pain. Journal of Bodywork and Movement Therapies, 8(2), 143–153.
Mense, S. (2008). Muscle pain: mechanisms and clinical significance. Deutsches Ärzteblatt International, 105(12), 214–219.
Myers, T. W. (2004). Anatomy Trains. Elsevier Urban & Fischer.